Laryngeal Cancer: Staging and Treatment
What is staging for cancer?
Staging is the process of learning how much cancer is in your body and where it is. For laryngeal cancer (cancer of the larynx/voice box), tests like laryngoscopy, endoscopy, fine needle aspiration, barium swallow, CT, MRI, and/or PET scans may be done to help stage your cancer. Your provider will look at the size of your tumor, where it is, and if it has spread to other organs to help figure out the stage. Staging helps guide the best treatment plan for you.
How is laryngeal cancer staged?
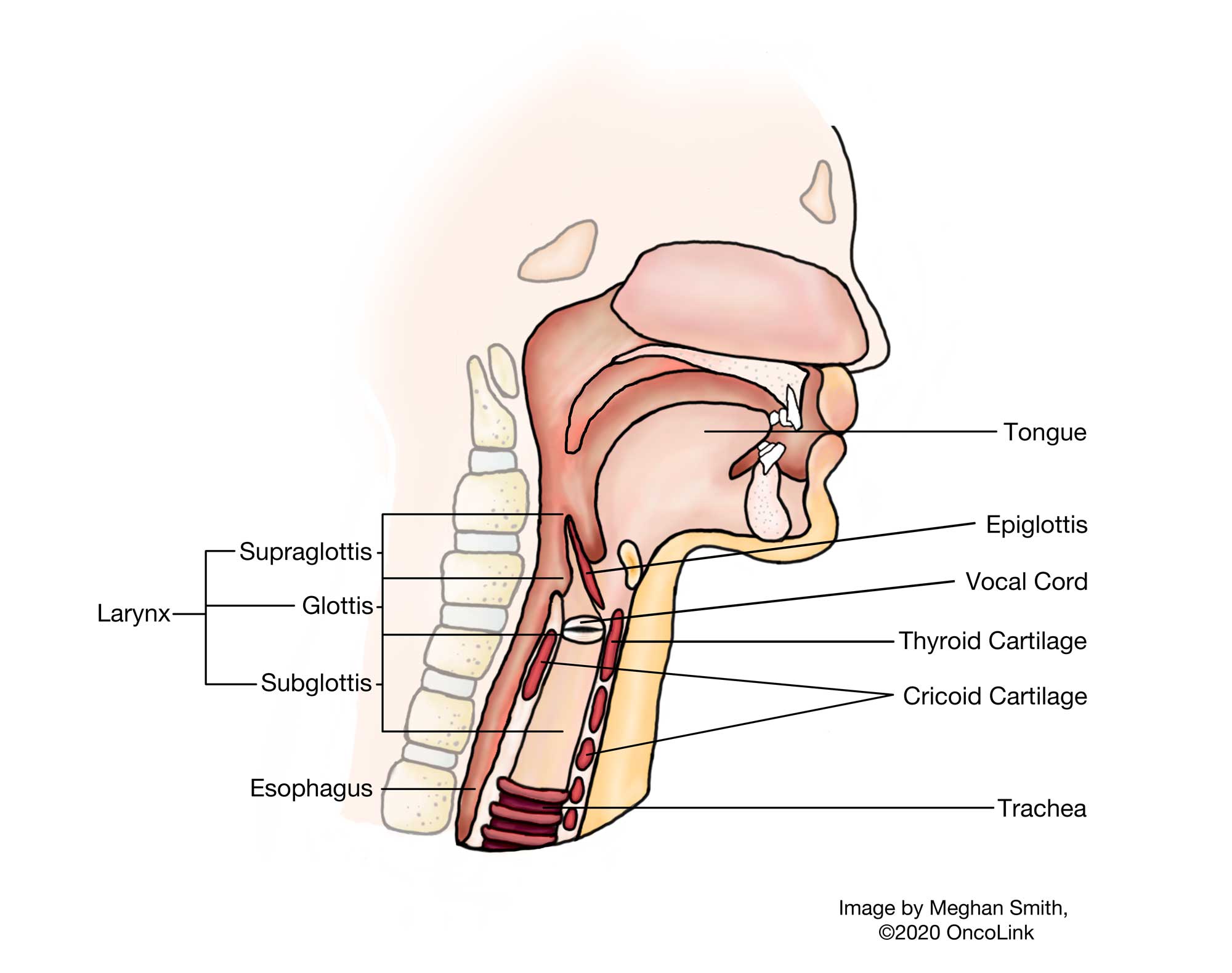
Laryngeal cancer affects your voice box and the epiglottis (cartilage that protects your larynx). The staging of laryngeal cancer is based on where in the larynx the cancer starts. There are three parts of the larynx:
- Supraglottis: The area above the vocal cords.
- Glottis: The area that includes the vocal cords.
- Subglottis: The area below the vocal cords.
Staging is also classified using the American Joint Committee on Cancer’s “TNM system”:
- T- Describes the size/location/extent of the "primary" tumor in the larynx (voice box).
- N- Describes if the cancer has spread to the lymph nodes.
- M- Describes if the cancer has spread to other parts of the body (metastasized).
Your provider will use the results of the tests you have to find your TNM and combine these to get a stage from 0 to IV (4).
Staging is important because it helps guide your treatment options. The staging system is very complex. Below is a summary of the different stages. Talk with your provider to learn more about your specific cancer and its stage.
Stage 0 (Tis, N0, M0): The tumor is only on the surface of the cells in the larynx and has not spread to any lymph nodes or other parts of the body.
Stage I (T1, N0, M0)
- Supraglottis laryngeal cancer: The tumor is on one part of the larynx called the supraglottis and your vocal cords are not affected.
- Glottis laryngeal cancer: The tumor is on the vocal cords but has not changed the ability of the vocal cords to move (this produces sound/speech).
- Subglottis laryngeal cancer: The tumor is only affecting the subglottis.
If your cancer is stage I, it has not spread to any lymph nodes or other parts of the body (has not metastasized).
Stage II (T2, N0, M0)
- Supraglottis laryngeal cancer: The tumor is in more than one part of the supraglottis or glottis (vocal cords) OR is outside of the supraglottis near the base of your tongue or the wall of the sinuses and is not attached to the larynx. It has not spread to any lymph nodes or other parts of the body.
- Glottis laryngeal cancer: The tumor is in the glottis and has grown to the supraglottis and/or subglottis. The ability of your vocal cords to move and produce sound/speech is also affected.
- Subglottis: The tumor is in the subglottis and has also grown to the vocal cords. The ability of your vocal cords to move may or may not be affected.
Stage III (T3, N0, M0), (T1, N1, M0), (T2, N1, M0), (T3, N1, M0)
- All types: The tumor is located within the larynx and the vocal cords cannot move; OR the tumor has grown to other locations within the larynx or thyroid cartilage. The tumor may have also spread to one or more lymph nodes on the same side of the neck as the tumor and is not larger than 3 centimeters (cm). It has not spread to other parts of your body.
Stage IVA (T1, N2, M0) (T2, N2, M0) (T3, N2, M0) (T4a, N0/N1/N2, M0)
- All types: Moderately advanced local disease. The tumor may be growing into cricoid and/or thyroid cartilage or areas of your trachea, neck, tongue, thyroid, or esophagus. The tumor may have also spread to one or more lymph nodes on the same side of the neck as the tumor and is 3 to 6 cm. It has not spread to other parts of your body.
Stage IVB (Any T, N3, M0) (T4b, Any N, M0)
- All types: Very advanced local disease. The tumor may be growing into prevertebral space (deep part of your neck), might surround the carotid artery, or grow into your mediastinum (upper belly and chest area). The tumor may have spread to one or more lymph nodes, may be larger than 6 cm, and/or may break through the outer capsule of the lymph node. It has not spread to other parts of your body.
Stage IVC (Any T, Any N, M1)
- All types: Very advanced local disease. The tumor may be growing into prevertebral space (deep part of your neck), might surround the carotid artery, or grow into your mediastinum (upper belly and chest area). The tumor may have spread to one or more lymph nodes, may be larger than 6 cm, and/or may break through the outer capsule of the lymph node. The cancer has spread to other organs.
How is laryngeal cancer treated?
Treatment for laryngeal cancer depends on many things, like your cancer stage, age, overall health, and test results. There are steps to take before treatment can begin for any kind of head and neck cancer:
- Multidisciplinary treatment is very important. This means you will have providers from many different specialties (this could include: cancer/oncology, radiation, nutrition, and others) on your care team. Many of these providers will see you before you start treatment during visits called consultations. They will work together and with you to make a treatment plan.
- If you smoke, quit as soon as possible. Smoking may affect how well your treatments work and can worsen side effects.
Your treatment may include:
- Surgery.
- Radiation Therapy.
- Chemotherapy.
- Targeted Therapy.
- Immunotherapy.
- Supportive/Palliative Treatment.
- Clinical Trials.
Surgery
The goal of surgery is to remove all or as much of the cancer as possible. Your surgeon will also try to avoid damage to other tissue or organs near the tumor. There are a number of surgical options to treat cancer of the larynx. Possible surgical treatments for laryngeal cancer can be:
- Vocal Cord Stripping: The top layers of tissue on the vocal cords are stripped away using a long surgical tool. This is used to biopsy or treat stage 0 cancer. After recovery, you often still have your normal speaking voice.
- Cordectomy: Part or all of your vocal cords are removed. How much this affects your ability to talk depends on how much of the vocal cord is removed. If only part of the vocal cord is removed, you may have hoarseness. If both cords are removed, you will not be able to speak normally.
- Laryngectomy: There are a few types of laryngectomies.
- Partial Laryngectomy: Used if there is a smaller tumor. Only part of the larynx is removed. There are two types:
- Supraglottic laryngectomy: The part of the larynx above the vocal cords, known as the supraglottis, is removed. You will be able to speak normally after surgery.
- Hemilaryngectomy: Used for smaller tumors of the vocal cords, involves the removal of one side of the larynx (and one vocal cord). Because some vocal cord remains, you will still be able to talk after, but your voice may change.
- Total Laryngectomy: Used in advanced cancers, the entire larynx is removed. The windpipe (trachea) will be brought up through the skin on the front of the neck, making a hole (stoma) that you will now breathe through, rather than through your nose or mouth. This is known as a tracheostomy. You will not be able to speak normally. After recovery from the surgery, you should be able to swallow normally.
- Partial Laryngectomy: Used if there is a smaller tumor. Only part of the larynx is removed. There are two types:
- Laser Surgery: In laser surgery, an endoscope (a thin tool that has a light and camera on it) is placed into your mouth and down your throat to find the tumor. A laser is used to vaporize or cut it out (excise). You may have a hoarse voice.
- Lymph Node Dissection: You may have one or a few lymph nodes removed along with nerves and muscle. Your surgeon will decide what needs to be removed based on your needs.
If the cancer has grown into your throat, you may have a partial or full pharyngectomy, which is the removal of the throat. If the cancer has affected your thyroid, you may need a thyroidectomy.
Radiation Therapy
You may need radiation therapy. Radiation therapy uses high-energy X-rays to kill cancer cells. Radiation may be used as the only treatment or in combination with surgery and/or chemotherapy. Early-stage laryngeal cancer may be treated with radiation alone. This can preserve better voice quality for some patients. When radiation is used with surgery, it is called adjuvant therapy. Radiation may be used after surgery to kill any remaining cancer cells and to lower the chance of recurrence (your cancer coming back). Radiation may also be used if you cannot have surgery or to help control symptoms, such as pain and bleeding. It can cause side effects such as skin irritation and it can affect nearby glands and tissues.
Chemotherapy
Chemotherapy is the use of anti-cancer medicines that go through your whole body. These medicines may be given through a vein (IV, intravenously) or by mouth.
Chemotherapy is used to treat laryngeal cancer if it has spread (metastasized) or if the cancer was not completely removed during surgery. The chemotherapy medications commonly used to treat laryngeal cancer are cisplatin, carboplatin, fluorouracil, docetaxel, paclitaxel, methotrexate, capecitabine, and epirubicin.
Targeted Therapy
Laryngeal cancer may be treated with targeted therapies that focus on specific gene mutations or proteins in the tumor. Targeted therapies work by targeting something specific to a cancer cell, which lets the medication kill cancer cells and affect healthy cells less. Sometimes the “target” is also in healthy cells and side effects can happen as a result. An example of a targeted therapy used for this type of cancer is cetuximab.
Immunotherapy
Immunotherapy is the use of a person's own immune system to kill cancer cells. Immunotherapy medications that may be used to treat this type of cancer are pembrolizumab and nivolumab. Your tumor may need to be tested to make sure immunotherapy medications will work for you.
Possible Side Effects
Your quality of life is very important during and after treatment. Supportive and palliative treatments are used to lessen symptoms or side effects that you may have. Head and neck cancer treatment and the cancer itself can cause:
- Pain: Your care team will help you with medications and other therapies for pain. Radiation, surgery, and a nerve block can help with pain as well.
- Nutrition issues: For some patients, trouble swallowing, mucositis (sore mouth and throat), loss of taste, or a lack of saliva production may make eating hard or impossible. You should see a dietitian who can help you with food and supplement choices. If needed, a speech and swallowing specialist can test if you can swallow safely without choking or inhaling food. Many patients will need to be fed through a tube placed in their stomach (called a PEG or ‘G' tube). In most cases, this is only temporary (for a short time).
- Personal and family changes: You may have changes with your body that could affect how you think about yourself (body image). Your cancer and treatment may also affect your role in your family. Social workers and psychologists can support you with both of these changes.
- Speech problems: A speech therapist can help you keep or get back as much of your speech as possible, and can teach you other ways to communicate.
Clinical Trials
You may be offered a clinical trial as part of your treatment plan. To find out more about current clinical trials, visit the OncoLink Clinical Trials Matching Service.
Making Treatment Decisions
Your care team will make sure you are included in choosing your treatment plan. This can be overwhelming as you may be given a few options to choose from. It feels like an emergency, but you can take a few weeks to meet with different providers and think about your options and what is best for you. This is a personal decision. Friends and family can help you talk through the options and the pros and cons of each, but they cannot make the decision for you. You need to be comfortable with your decision – this will help you move on to the next steps. If you ever have any questions or concerns, be sure to call your team.
You can learn more about laryngeal cancer at Oncolink.org.